
May 2007
Investigation of Airplane Seat Comfort (pilot test)
Methods
Five healthy participants (3 male, 2 female) aged 25.6 years (s.d. 3.78), were 1.78 m tall (s.d. 0.06) and had a mass of 78.7 kg (s.d. 15.4) participated in this study.
Pressure Maps Behind back and Under Buttocks and Thighs
One pressure mat was attached to the seat pan, and another attached to the seat back. Pressure was collected throughout the entire half hour collection time
Spine Curvature
Participants had two 3-space sensors attached to their back, sensor 1 at T-12/L1 and sensor 2 placed on their sacrum. The difference between the two sensors corresponded to the spine curvature. The 3space source was mounted externally in the same orientation as the two 3-Space sensor, and was placed one meter in front of the subject. Three-space was collected for 1 minute at the beginning of the study (time 0), then 15s at 5, 10 and 15 minutes. This sequence was repeated for both conditions of the study.
Condition 1
Participants were instructed to sit in the seat, and once they felt comfortable, the pressure and the first spine curvature collection began. Participants were instructed to not put their feet further than a taped line which represented the amount of leg room they would have in an actual flight. Collection time lasted 15 minutes.
Condition 2
Participants were instructed to sit in the seat, and place an inflatable lumbar support (lumbair) in the middle of their sacrum and lumbar spine, and inflate the lumbair to a “comfortable” level. Data collection followed the same procedure as in condition 1.
Condition 1 and 2 were randomized for each participant.
Results
Spine Angle
Spine flexion was significantly larger at the beginning of condition 1 (without the lumbair) than at the beginning of condition 2 (with the lumbair), as well as at after 5, 10 and 15 minutes of sitting (F = 6.24, p = 0.0085). Also at the start of condition 1, the spine angle is significantly less flexed than after 10 and 15 minutes of sitting without the lumbair (F = 6.24, p = 0.0085). There are no significant differences in the spine angle over the 15 minute trial when using the lumbair.
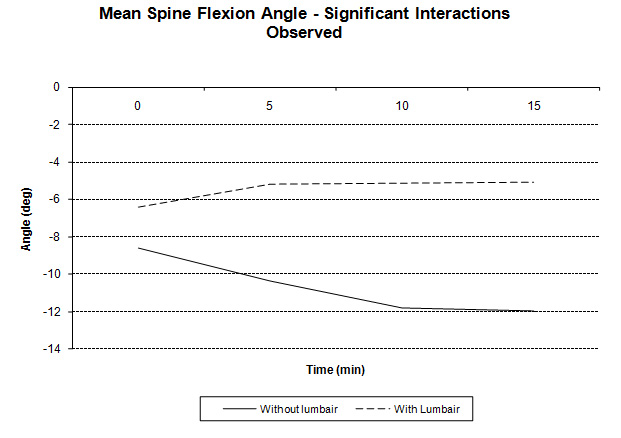
Figure 1: Illustration of the change in spine flexion over the fifteen minute trial with and without the lumbair.
Interpretation:
The lumbair keeps a more neutral spine curvature throughout the 15 minute trial. Conversely, without the use of the lumbair the spine creeps into further flexion for the first 10 minutes of sitting. This could mean that the lumbair helps to eliminate creep of the spine into flexion while sitting in the airplane seats.
Sitting Pressure:
The use of the lumbair influences pressure distribution over the back and underneath the buttock and thighs. With the lumbair in place, very little pressure is observed on the back rest, and more pressure, accompanied by an increase in the area of contact, is placed on the buttock and thighs. The center of pressure (COP) changes little as the majority of the pressure is located proximal and medially on both thighs as well as the anterior portion of the ischial tuberocity. The main difference is that it appears that the lumbair causes a shift in the weight from the back rest to the seat pan. Although it must be noted that one subject had an increase in pressure located at the shoulder with the use of the lumbair.
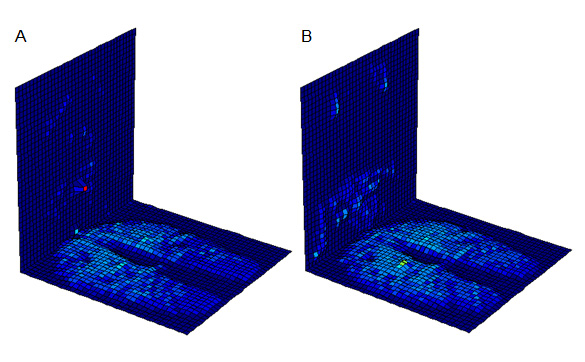
Figure 1: Pressure readings from the back of the seat and the seat pan for A. with no lumbair use, and B. with the use of the lumbair
Future Consideration
10 male and 10 female subjects, test for gender effects, and greater statistical power.
Longer collection time – half hour with for each condition
Testing people with a history of back pain.
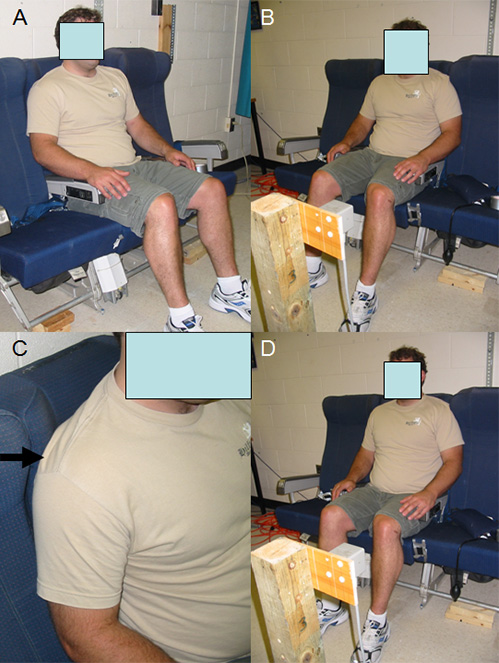
Figure 2: Illustration without the use of the lumbair (A,B) and the shoulder pressure created by the use of the lumbair (C) as well as the position adopted using the lumbair.
Using a Pneumatic Support to Correct Sitting Posture in Airline Seats
*Stuart M. McGill, PhD, Chad M.J. Fenwick, BSc
Spine Biomechanics Laboratories,
Faculty of Applied Health Sciences,
Department of Kinesiology,
University of Waterloo, Waterloo, Ontario, Canada, N2L 3G1
*Corresponding Author
Spine Biomechanics Laboratory
Department of Kinesiology
University of Waterloo
200 University Ave West
Waterloo, Ontario, Canada N2L 3G1
Tel: 519-888-4567 Ext. 36761 Fax: 519-746-6776
Submitted to Ergonomics
March 2008
Revision August 2008
Acknowledgements: We thank the Natural Science and Engineering Research Council of Canada (NSERC) for their financial support.
Ethics Review Board: Committee for research on humans, Office of Research Ethics, University of Waterloo
ABSTRACT
Prolonged sitting with spine flexion has been linked to low back disorders. A variety of mechanisms account for this based on biomechanical and neurological variables. Airline seats typically cause pronounced lumbar flexion due to their hollowed seat back design. A pneumatic support, placed between the seat back and the lumbar spine, was tested to see if lumbar flexion was reduced. Results showed that when the seats were positioned in the upright position, 15 of 20 participants experienced reduced lumbar flexion (15 degrees on average) with the support. The study was repeated on the 5 non-responders with the seatback set in the reclined position. This resulted in another 4 experiencing less lumbar flexion. Reducing flexion with the support reduces lumbar stress.
Statement of Ergonomic Relevance: While it is not known why airline seats are designed with no lumbar support which causes excessive lumbar flexion while seated, the pneumatic support corrected this deficit. Reclining the seatback enhances this effect.
Keywords: lumbar, support device, range of motion
INTRODUCTION
Posture of the lumbar spine while sitting is important for a number of reasons. Biomechanical evidence has shown that prolonged seated flexion causes creep in the posterior spine tissues (McGill and Brown, 1992), which has been documented to cause muscle spasms (Williams et al, 2000) and diminished extensor muscle reflex (Solomonow et al, 2003). These have been shown to occur within just 15 minutes of sustained flexion. Further, McGill and Brown (1992) observed that the joint laxity caused by flexion lasted for a substantial period of time such that spine stability would be compromised during subsequent activity (Beach et al, 2005), for example, when lifting baggage from an airport carrousel following a flight. Static sitting with a flexed spine results in higher intradiscal pressures (Wilke et al, 1999) probably due to the tensile forces imposed on the joint from posterior annulus and ligamentous strain (Hedman and Fernie, 1997). Repeated flexion has been shown to instigate discs herniation (Callaghan et al, 2001), while extension has been shown to be able to reverse partially herniated nucleus through the posterior part of the annulus (Scannell and McGill, in press). Interestingly, Alexander et al (2007) documented migration of the nucleus volume within the disc with flexed sitting concluding that sitting increases the risk of posterior disc derangements. More recent work has suggested that the majority of flexion when sitting occurs at the L5 disc thus concentrating stresses at this region (Dunk and Callaghan, Submitted). Even when sitting upright, videoflouroscopy evidence showed the L5 disc to be at 60% of full flexion, while all lumbar joints were close to full flexion when sitting slouched. They also concluded that flexion bending of the L5 disc was driven by the inclination of the pelvis. Proprioception evidence from Dolan and Green (2006) suggests there is a loss in the ability of people to regain a neutral lumbar posture following short bouts of slouched sitting. Specifically, this is a compromise of the ability to obtain a neutral spine posture for activities that follow a period of slouched sitting. This is important since the tolerance of the spine to bear load is highest when the spine has neutral curves (Gunning et al, 2001), neither flexed or extended. . There are plenty of epidemiologically based studies most of which link sitting with increased back disorders, particularly disc disorders (eg, Wilder et al 1988, Videman et al, 1990) but not all. However it is problematic to surveil “non-specific” back pain as there are those who will be relieved with sitting (perhaps those classed as extension intolerant, or who spend a large proportion of their time standing for example) and those catagories that are exacerbated by sitting (those who spend a large proportion of their time already sitting, those classed as flexion intolerant, or certain types of stenosis patients for example). Thus epidemiological reviews of non specific back pain only reach a conclusion based on the average of a non-homogenious group. Clinical evidence has shown many individuals with low back pain are exacerbated with prolonged sitting yet find frequent posture changes relieving together with work that does not cause spine flexion (McGill, 2007). It would appear that sitting is problematic for those who fall into the discogenic category for back pain genesis. Thus, evidence obtained from several perspectives suggests that avoidance of a loss of lumbar lordosis when sitting would be beneficial. Consequently, attempts to either directly influence the lumbar curve with a mechanical support, or support the pelvis in such a manner to influence its sagittal orientation and thereby lumbar curve, would be justified.
Airline seats, for some reason, often have a back rest contour that does not support the lumbar spine. Rather, the low back region of the seat back is hollowed causing the lumbar spine to flex. In addition, because a single non-adjustable design is used, there are often bolsters, higher in the seat back, that push the shoulders and upper torso forward in taller people. This results in further lumbar spine flexion. No scientific rationale for this design could be uncovered except that some designers may have been misguided into believing that seat design to flex the spine is comfortable. Preserving a more neutral curve while seated appears justifiable, particularly during prolonged sitting associated with airline travel. Furthermore, passengers are often required to sleep in such a posture. In summary, there appears to be sufficient evidence from several perspectives that document the detrimental effects of prolonged flexed sitting together with modulating the risk of back injury following flexed sitting, such as lifting luggage. Attempts to reduce lumbar flexion during airline travel would appear worthy of consideration, and probably essential for those with lumbar flexion intolerance.
This study evaluated the ability of a pneumatic support, placed in the low back of people seated in a typical airline seat, to influence the lumbar curve. It was hypothesized that the support could correct the lumbar spine towards a more neutral posture. Lumbar spine curvature was documented both with, and without, a pneumatic support, together with the pressure distribution over the backrest and seat pan of the airline seat.
METHODS
Experimental methods and procedures were approved by the University Office of Human Research Ethics. Twenty healthy participants (10 male, 10 female) were recruited from the university undergraduate and graduate population to participate in this study (male averages: age 26.1 yrs. (s.d. 2.7), Height 181.8 cm. (s.d. 3.9), Weight 84.4 kg. (s.d. 9.2) (female averages: age 24.4 yrs. (s.d. 3.9), Height 163.7 cm. (s.d. 8.4), Weight 60.7 kg. (s.d. 2.9).
Spine Curvature
Participants had two 3-space sensors (3 Space Isotrak, Polhemus Navigation Systems, Colchester, Vermont) attached to the midline of their back, sensor 1 at T-12/L1 and sensor 2 placed on their sacrum. The angular difference between the two sensors, sampling at 30Hz, corresponded to the spine curvature. The system was “zeroed” in a standing posture corresponding to zero degrees of flexion. This angular data was collected over a 15s window at the beginning of the study (time 0), and again at 5 minute intervals for a total of 30 minutes. This sequence was repeated for both conditions (with support, without support) of the study.
Pressure Mats Behind back and Under Buttocks and Thighs
Pressure mats (Model x36, X Sensor Technology Corporation, Calgary) were placed over the seat pan and back of the airline seat to document the distribution of forces on the thighs, buttocks and backs of the participants. Pressure readings were sampled and collected at 4 Hz throughout the entire half hour collection time for each condition. Pressure was displayed on the computer screen with different colours corresponding to different levels of pressure. In this way a pressure “contour” map was created.
Experimental Conditions: With and Without the Support
Conditions (with and without the support) were presented in a randomized order for the participants. Participants sat in the airline seat, and once they felt comfortable, collection of person-seat interface pressure and spine curvature began. Room in front of the chair was restricted to represent the amount of leg room they would have during an actual flight. The first collection time lasted 30 minutes.
In the condition where a lumbar support was tested, participants sat in the seat, with their pelvis to the rear of the seat pan. Then an inflatable lumbar support (LumbairPlus, Innotech Rehabilitation Products Inc., Orillia, Ontario) was placed in the middle of the lower part of their lumbar spine, and inflated to a “comfortable” level (see Figure 1). Another half hour of data was collected. One hour of sitting had then elapsed (30 minutes with, and 30 minutes without, the support).
At this point, participants were instructed to over inflate the pneumatic support to see how much further it was capable of driving the lumbar spine into extension. Following this, participants filled out a comfort questionnaire of 3 questions: “Is the airline seat comfortable?”; “Did the pneumatic support add any comfort”; “Would you purchase the pneumatic support?”
Data Analysis
Spine flexion angle was calculated as the average flexion angle over the middle 5 second portion of each data sample. These angles were assessed using a three way repeated measures analysis of variance (ANOVA) (between factor gender: 2 levels; within factors condition: 2 levels; time: 7 levels, α = 0.05) followed by a Tukeys post hoc analysis.
Pressure maps were plotted for visual/qualitative analysis. In the final full inflation trial, spine flexion was recorded throughout for 30 seconds, and the minimum and maximum value used to calculate additional spine motion (if any).
Note that an unexpected result was obtained and that a second data collection was then conducted on a subgroup with the seatback of the airline seat set in the reclined position. At that point an ANOVA was conducted on the collected variables to see if there were any distinguishing features peculiar to a subgroup.
RESULTS
All participants sat in the airline seat with a flexed lumbar spine (23 degrees on average). This constituted some individuals sitting at 97% of their full spine flexion. There was no effect of gender so that data were collapsed for analysis. Comparing the lumbar spine posture between the two conditions (with and without the pneumatic support) and over each 30 minute session, the pneumatic support reduced the lumbar flexion (to just under 15 degrees, p=0.01). However, not all participants experienced a reduction in lumbar flexion as 5 of the 20 participants increased their lumbar flexion further (known as the non-responders). To be clear, 15 experienced a lessening of spine flexion (the responders), which was an expected result, while 5 actually experienced more flexion. All further analysis was conducted based on these two sub-groups.
In the no support condition the responders (those who experienced their spines extended towards neutral with the support) began sitting with 26 degrees of lumbar flexion (figure 2). This settled to 27 degrees by the end of the 30 minutes with no support. In contrast the non-responders began sitting with less flexion (13.5 degrees) (p<0.0001) and this did not change over the 30 minutes. With the support, the responders experienced less spine flexion (11 degrees of flexion compared to 26 degrees without the support) at the beginning of the trial but settled at 12 degrees by the end of 30 minutes. Thus, the support reduced sitting flexion 15 degrees moving the spine towards a more neutral posture. In contrast, the non-responders experienced more flexion with the support (from 13.5 to 25 degrees) which settled to 26 degrees by the end of the 30 minutes (Figure 3).
There was no consistent trend in the full inflation trial nor did any participant report that they would naturally do this. No further analysis was conducted in this regard.
Qualitative analysis of the pressure maps revealed patterns of pressure concentrations over the ishial tuberocities with distributed patterns over the soft tissues of the thighs and buttocks (Examples are shown in Figure 4). However, we were unable to determine any link between a specific pattern of pressure and the nature of the response to the support. Pressure concentrations increased over the 30 minutes in both the no support, and the support conditions.
Questionnaire results revealed that the unaltered airline seat was perceived as clearly uncomfortable by 9 participants while only 2 rated it as comfortable. The remaining participants qualified their responses as moderately comfortable/uncomfortable but that comfort declined over time. There was no link between perceived comfort of the chair and whether they were responders or non-responders. In answering the question, “Did the support add any comfort?”, 13 stated yes, 5 stated no, while 2 qualified their answers stating that they would not use it continuously for long periods. Interestingly, of the 5 non-respondents only 1 stated it did not add comfort. In answering the question “Would you purchase the support?, 9 stated “yes”, 9 stated “no”, and 2 stated possibly. This may be biased in that some who stated that they would not buy the support noted that they would use other forms of support such as a pillow or rolled up jacket (given that they were students and these were cheaper alternatives).
Follow Up Study:The binary response to the support that created the two groups – those that increased lumbar flexion and those that increased extension, was not anticipated. Logically, placing a support behind the lumbar spine was only anticipated to cause lumbar extension. To investigate what possible mechanism could result in lumbar flexion the non-responders were asked to return to the laboratory several weeks following the first session. Quantification of these non-responders revealed that the lumbar support pushed the entire torso forward causing the increase in lumbar flexion (ie, the whole spine slumped forward into more flexion in the 5 non-responders). From observation, it became clear that the seat back of the chair was so upright in its normal position that it placed the centre of mass of the upper body close to the support line passing down through the hips. Note that the height of the participant was not linked to their response. The experiment was then repeated on the non-responders with the seat back in the reclined position (from 110 to 125 degrees measured between the seat pan to seat back) (see figures 5 and 6). This changed the response. In 4 of the former non-responders, the pneumatic support created extension to move the spine towards a more neutral posture, reclassifying them into responders.
DISCUSSION
The placement of a pneumatic support in the lumbar region while sitting in a typical airline seat reduced lumbar flexion. However, the hypothesized result needs qualification in that 15 of 20 participants reduced lumbar flexion with the seat back in an upright position, and 19 of 20 experienced a reduction with the seat back in a reclined position. This appeared to be due to the moving of their upper body centre of mass posteriorly so that the lumbar support then created a 3 point bending force and lumbar extension.
There was no existing data on airline seats that we were able to find to compare with the findings of this study.
This study observed people with the pneumatic lumbar support for periods of 30 minutes. We do not know if the effect would be maintained for more prolonged flights. However, the design of the device we tested had a convenient pump and relief valve that is placed in the lap of the user to promote regular adjustments to the pressure, and therefore spine posture. We did observe an asymptote to the spine posture function after a few minutes suggesting that the posture is driven by the support and that flexion creep occurs in the first few minutes of introducing the support.
In summary, airline seats cause a flexed lumbar posture (up to 97% of full lumbar flexion in some people). The pneumatic lumbar support did influence lumbar posture into positions that have been shown to reduce stress on the vulnerable components of the lumbar spine –namely the posterior annulus of the disc and ligaments. Further, reducing prolonged lumbar flexion would avoid the suspected complications from prolonged flexion such as detrimental muscle reflex modulation and exacerbation of disc herniation and prolapse. This would be particularly important for people who have back pain provoked by flexion – or are classified as being flexion intolerant. Flexion not only induces pain but also reduces their tolerance to other loading modes such as compression and shear (the interested reader is referred to Magee, 1997, and McGill, 2007, for clinical tests to identify and correct these individuals). It is not known why airline seats are designed with a hollowed lumbar region when this is deemed both uncomfortable by many, and results in increased stress in the vulnerable spine. However, the pneumatic support does move the spine towards a tissue unloading posture, particularly when the seat back is reclined. This not only reduces stress while sitting but also may prepare the spine following a period of prolonged sitting when a demanding lift may be required – such as picking luggage from an airport carrousel.
REFERENCES
Alexander, L.A., Hancock, E., Agouris, I., Smith, F.W., MacSween, A., (2007) The response of the nucleus pulposus of the lumbar intervertebral discs to functionally loaded positions, SPINE, 32:1508-1512.
Beach, T., Parkinson, R., Stothart, J., Callaghan, J., (2005) Effects of prolonged sitting on the passive flexion stiffness of the in vivo lumbar spine, The Spine J., 5:145-154.
Callaghan, J.P., and McGill, S.M. (2001) Intervertebral disc herniation: Studies on a porcine model exposed to highly repetitive flexion/extension motion with compressive force. Clin. Biom. 16(1): 28-37.
Dolan, K.J., and Green, A., (2006) Lumbar spine reposition sense: The effect of a “slouched” posture, Manual Therapy, 11:202-207.
Dunk, N., and Callaghan, J.P., (submitted) Sagittal lumbo-sacral intervertebral angles in seated postures using digital radiography – Evidence of a pelvis driven flexion pattern.
Gunning, J.L., Callaghan, J.P. and McGill, S.M. (2001) The role of prior loading history and spinal posture on the compressive tolerance and type of failure in the spine using a porcine trauma model. Clin. Biomech. 16(6): 471-480.
Hedman, T.P., and Fernie, G.R., (1997) Mechanical response of the lumbar spine in seated postural loads, SPINE, 22:734-743.
Magee, D.J., (1997) Physical orthopaedic assessment, W.B. Saunders Company, Philadelphia.
McGill, S.M., and Brown, S. (1992). Creep response of the lumbar spine to prolonged full flexion, Clin. Biomech. 7: 43-46.
McGill, S.M. (1997). Invited Paper: Biomechanics of Low Back Injury: Implications on current practice and the clinic. J. Biomech. 30(5): 465-475.
McGill, S.M., (2007) Low back disorders: Evidence based prevention and rehabilitation, Second edition, Human Kinetics Publishers, Champaign.
Scannell, J.P., and McGill, S.M. (2003). Lumbar posture – should, and can, it be modified? A study of passive tissue stiffness and lumbar position in activities of daily living. Phys. Ther., 83(10): 907-917.
Solomonow, M., Baratta, R.V., Zhou, B-H., Burger, E., Zieske A., Gedalia, A., (2003) Muscular dysfunction elicited by creep of lumbar viscoelastic tissues, J. EMG, Kinesiol. 13:381-393.
Videman, T., Nurminen, M., Troup, J.D.G. (1990). Lumbar spine pathology in cadaveric material in relation to history of back pain, occupation, and physical loading, Spine, 15:728-740.
Wilder, D.G., Pope, M.H., Frymoyer, J.W. (1988). The biomechanics of lumbar disc herniation and the effect of overload and instability. Journal of Spinal Disorders, 1:16-32.
Wilke, H-J., Neef, P., Caimi, M., Hoogland, T., Claes, LE., (1999) New in vivo measurements of pressures in the intervertebral disc in daily life, SPINE, 24:755-762.
Williams, M., Solomonow, M., Zhou, B-H., Baratta, R.V., Harris, M., (2000) Multifidus spasm elicited by prolonged lumber flexion, SPINE, 25:2916-2924.
Figure Captions:
Figure 1: A pneumatic support (A) was placed in the lower lumbar region (B). It has a bladder where the inflation level is controlled by the user with a pump and release valve that is placed in the lap of the user. The intent is to reduce lumbar flexion towards a neutral spine posture (C).
Figure 2: Average lumbar flexion angle over the 30 minute trial both with and without the pneumatic support for the 15 responders. On average, there was a slow creep towards more flexion over the trial. The support reduced lumbar flexion approximately 15 degrees.
Figure 3: Average lumbar flexion angle for the 5 non-responders. While they began the trial with less flexion than the responders, the support caused more lumbar flexion.
Figure 4: Pressure distribution over the seat pan (left panel) and chair back (right panel) in a single participant. Lighter areas denote higher pressure. A) at the beginning of the 30 minute trial without the support; B) at the end of the no support trial; C) at the beginning of the support trial; D) at the end of the support trial. Stress concentrations develop over the 30 minutes as seen by the lighter areas (more lightness seen in B compared to A, and in D compared to C) but there was no pattern to distinguish between the support, or no support condition.
Figure 5: The initial experiment was conducted with the seat back upright (110 degrees). A) the average posture adopted by all when sitting in the seat without a support; B) the average spine posture when inflating the support adopted by the “responders”; C) the average spine posture when inflating the support adopted by the “non-responders”.
Figure 6. The experiment was then repeated on the non-responders with the seat back in the reclined position (from 110 to 125 degrees measured between the seat pan to seat back). In the first experiment the support pushed the entire torso forward causing spine flexion in the non-responders however when the seat was reclined the support then created a better 3-point bend to cause spine extension.